In its analysis, the foundation accounted and adjusted for a host of patient characteristics that might skew the numbers. Still, the broad variation is there. Shannon pointed out that it would be "unusual" that patients would differ so significantly in what treatments they wanted, simply according to where they lived.
"It's much more likely," Shannon said, "that physicians practicing in that area tend to rely on that course of treatment over others. ... It does seem to be more the physician preference than the patient preference."
Professor Renee Hsia at UC San Francisco was not involved in the study. She agreed that physician preference matters, counter to what patients might think.
"A lot of patients out there think you go to one doctor and they will prescribe the same treatment," no matter where you live, Hsia said, "because you go to medical school and there's one answer." Tuesday's release shows there's "a lot of variability."
"The way your peers practice ... in your group or in your hospital affects the way you practice also," Hsia said. "I wouldn't say it's peer pressure, but it's adapting to your current environment."
Patients should be "good consumers"
Jeff Belkora, a UCSF professor of health policy says that physician preference for certain treatments needs to be "trumped" by what individual patients need. He called for patients to be good consumers and challenge their physicians. "We want to work with our physicians," Belkora said. "We want to trust them. At the same time ... any given doctor is different than any given patient, so we need to make them understand what we want and what we need."
If you're thinking that's a tall order in the face of a challenging diagnosis, patients should remember that they likely have more time to weigh options than they might think. Belkora says patients need to make their diagnosis and treatment decisions into a "project."
Elizabeth Becker of Piedmont did exactly that. She was diagnosed with DCIS, a very early stage non-invasive breast cancer, a year ago. She spent weeks researching her treatment options. The more she found out about the specific biology of her specific type of cancer, the closer she came to a decision. While DCIS is unlikely to recur as invasive cancer, in Becker's case, if the cancer recurred, it was likely to be aggressive. Becker ultimately chose a mastectomy.
"I felt powerful," she said, referring to the process of deciding as well as the options and choices she had. She also credited her doctor who held open-ended conversations with her. Becker said another doctor she had seen seemed to want to "teach me about breast cancer and then tell me my (treatment) option." She was unimpressed.
Belkora says there are resources available for people facing treatment decisions. The first stop is research at reputable sites such as the American Cancer Society or the National Cancer Institute for those with a cancer diagnosis, he says.
The Informed Medical Decisions Foundation has decision aids for a wide variety of conditions, from cancers to back pain to heart disease. Health libraries at medical centers can also be a good resource.
But it's easy to imagine that handling this "project" and doing all this research is a tall order for anyone staring down a diagnosis, let alone the most vulnerable among us, people who are low income, with little education, people who have limited English skills.
While Shannon said the foundation's goal is in part to encourage patients to be more proactive, she also said the greater transparency could be an effective way to let "physicians know that they seem to be outliers," she said. "that they seem to be prescribing a particular course of treatment much more often or less often than their peers across the state do."

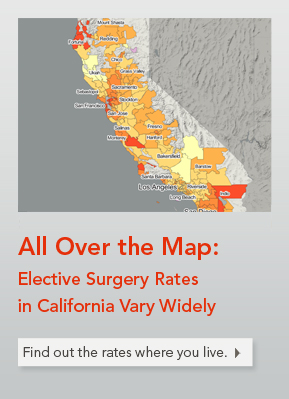 Low rates are easy to find, too. To name just one: women in Lancaster, northeast of Los Angeles, with early stage breast cancer receive lumpectomy with radiation at just 26 percent of the statewide average.
Low rates are easy to find, too. To name just one: women in Lancaster, northeast of Los Angeles, with early stage breast cancer receive lumpectomy with radiation at just 26 percent of the statewide average.